Pulmonary Hypertension: Symptoms, Right Heart Strain, and Therapy
When you start feeling out of breath climbing stairs, or notice your ankles swelling for no clear reason, it’s easy to brush it off. Maybe you’re just getting older. Maybe you’re not fit enough. But if these symptoms stick around-especially if they get worse over months, not days-you could be dealing with something more serious: pulmonary hypertension.
Pulmonary hypertension (PH) isn’t just high blood pressure in the lungs. It’s a slow, silent process where the arteries carrying blood from your heart to your lungs narrow and stiffen. That forces your right ventricle to work harder and harder, until it starts to strain, stretch, and eventually fail. Left untreated, it can be deadly. But with early detection and the right treatment, many people live full, active lives today.
What Pulmonary Hypertension Really Means
Normal pulmonary artery pressure is around 8-20 mmHg. When it stays above 20 mmHg at rest-measured directly through right heart catheterization-you’re diagnosed with PH. This isn’t just a number. It’s a sign that your heart is fighting against stiff, clogged vessels. The blood can’t flow easily, so your right ventricle has to pump harder. Over time, that muscle thickens, enlarges, and loses its ability to contract properly. That’s right heart strain.
PH isn’t one disease. It’s grouped into five types by the World Health Organization:
- Group 1: Pulmonary arterial hypertension (PAH)-the most severe, often genetic or idiopathic.
- Group 2: Caused by left heart failure-like from a weak left ventricle.
- Group 3: Linked to lung diseases-COPD, pulmonary fibrosis, long-term low oxygen.
- Group 4: Chronic blood clots in the lungs (CTEPH).
- Group 5: Unclear causes-like kidney disease, sarcoidosis, or blood disorders.
Knowing the group matters because treatment changes. Group 1 gets targeted drugs. Group 2 needs heart failure therapy. Group 4 might need surgery. Mislabeling it delays care.
Early Symptoms Are Easy to Miss
Most people don’t wake up one day with chest pain. PH creeps in. The first sign? Shortness of breath during normal activity. Not after running a marathon-after walking to the mailbox. Then comes fatigue. Then swelling in the legs or belly. Dizziness. Fainting. A racing heartbeat.
Doctors often mistake these for asthma, anxiety, or aging. A 2023 survey by the Pulmonary Hypertension Association found that 78% of patients were misdiagnosed for over a year. One man in Manchester thought he was just out of shape until his 6-minute walk distance dropped from 450 meters to 220 meters over 18 months. His GP said, “You need to exercise more.” A specialist later found his pulmonary pressure was 58 mmHg.
Physical exam clues matter too. A loud second heart sound (S2), a heave in the chest from the right ventricle pushing hard, or bulging neck veins (jugular venous distension) aren’t random. They’re signs your heart is under siege.
Right Heart Strain: The Hidden Killer
Pulmonary hypertension doesn’t kill because of lung damage. It kills because the right side of the heart gives out.
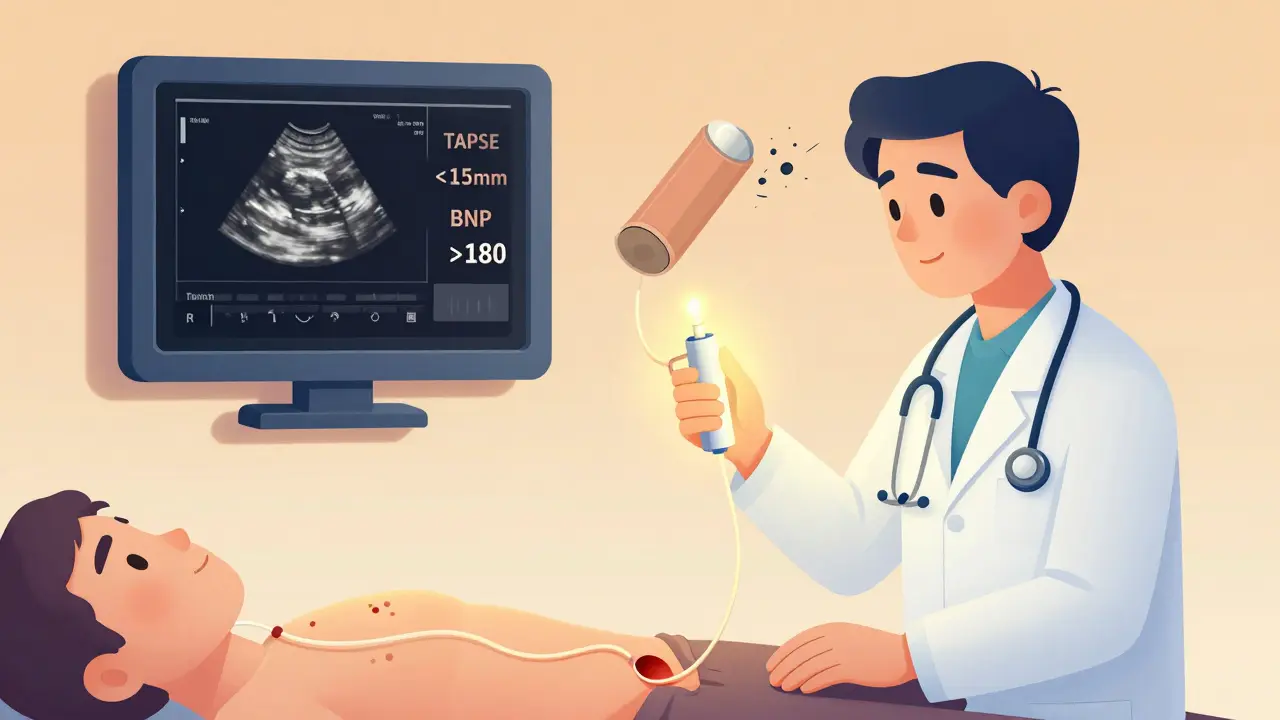
When the right ventricle strains, it changes shape. On echocardiogram, we look for:
- Wall thickness over 5 mm
- End-diastolic area bigger than 22 cm²
- TAPSE under 17 mm (that’s how far the valve moves during a beat)
If TAPSE falls below 15 mm, your risk of death in the next year doubles. BNP and NT-proBNP blood levels tell the same story. Above 180 pg/mL for BNP or 1,400 pg/mL for NT-proBNP? That’s a red flag. One study showed patients with NT-proBNP over 2,000 had a 70% chance of dying within 12 months without treatment.
The 6-minute walk test is simple but brutal. Walk as far as you can in six minutes. If you cover less than 380 meters, your prognosis worsens. A 2020 analysis found these patients were over twice as likely to die or need hospitalization. That’s not just a number-it’s a warning.
Diagnosis: Why Catheterization Still Matters
Echocardiograms are the first step. They’re non-invasive, quick, and widely available. But they’re not perfect. A 2019 study in Circulation found echocardiography overestimates pressure by 10-15 mmHg in over half the cases. That means people get falsely diagnosed-or worse, missed entirely.
Right heart catheterization is the gold standard. A thin tube is threaded from the groin or neck into the heart to measure pressure directly. It’s not risky for most. The chance of a serious complication? Less than 5%. But it’s still underused. Many clinics skip it because they rely on echo alone.
That’s a mistake. Dr. Nazzareno Galiè, who helped shape European guidelines, says: “Non-invasive methods cannot replace direct pressure measurement.” Why? Because only catheterization can tell if the problem is in the lungs (pre-capillary) or the heart (post-capillary). That difference changes everything.
Cardiac MRI gives the clearest picture of right ventricle size and function-but only 37% of PH centers in the U.S. have it. So most rely on echo, catheterization, and biomarkers together.
Therapy Has Changed Dramatically
Twenty years ago, PH meant a life expectancy of under three years. Today? Five-year survival is over 60%. That’s because we don’t treat PH with one drug anymore-we use combinations.
There are now 14 FDA-approved medications, grouped into five classes:
- Phosphodiesterase-5 inhibitors: Sildenafil, tadalafil-help relax arteries.
- Endothelin receptor antagonists: Bosentan, macitentan-block a chemical that narrows vessels.
- Prostacyclin analogs: Epoprostenol, treprostinil-mimic a natural vasodilator. Often given by IV or inhalation.
- Guanylate cyclase stimulators: Riociguat-boosts a signaling molecule that opens blood vessels.
- Sotatercept: Approved in 2021-first drug to target the root cause in PAH by rebalancing growth signals.
Before 2015, most patients got one drug. Now, 68% of PAH patients start on two or three together. That’s because studies show combination therapy cuts hospitalizations and doubles survival time.
For Group 4 (CTEPH), surgery to remove clots (pulmonary thromboendarterectomy) can be curative. For others, lung transplant remains an option-but it’s rare, complex, and reserved for the worst cases.

Why Care Needs to Be Specialized
PH isn’t something your local cardiologist can manage alone. It needs a team. A PH center includes:
- A pulmonologist who knows the disease
- A heart failure specialist
- A pharmacist who handles complex drug interactions
- A nurse coordinator who tracks labs, adjusts meds, and calls when something’s off
- A social worker to help with insurance and costs
One study showed PH nurse coordinators cut hospital stays by 27%. Why? Because they catch problems early. A patient’s BNP rises from 200 to 450? The nurse calls the doctor before the patient feels dizzy.
Only about 35 centers in the U.S. are certified to treat PH. In the UK, the number is even smaller. Many patients wait months just to get an appointment. And even then, insurance delays can hold up life-saving drugs. One survey found 63% of patients waited over 30 days for approval on IV prostacyclin.
What’s Next? The Future of PH Care
New tools are coming. The 2022 revision lowered the diagnostic cutoff from 25 mmHg to 20 mmHg. That means more people will be caught earlier. The LIBERTY trial is testing let-7 microRNA as a blood marker for early right heart damage-before symptoms show.
Drugs targeting the heart’s energy use are in trials. Dichloroacetate, for example, helps the right ventricle burn fuel more efficiently. Phase 2 results are expected late 2024.
But the biggest challenge isn’t science-it’s access. A 2023 report showed minority patients wait 47% longer for diagnosis and have 32% higher death rates. That’s not biology. That’s systemic failure.
The Pulmonary Hypertension Association’s 2025 plan aims to cut diagnostic delays to under a year. How? By training primary care doctors to recognize the red flags: progressive breathlessness, unexplained right heart thickening on EKG, swelling without heart failure. If you’re a GP and someone says, “I’m winded climbing one flight of stairs,” don’t tell them to exercise more. Ask: Have they been tested for PH?”
Can pulmonary hypertension be cured?
In most cases, no-but it can be managed effectively. Group 4 PH (caused by chronic blood clots) can sometimes be cured with surgery. For other types, especially Group 1, there’s no cure yet. But with combination drug therapy, many patients live 10, 15, or even 20 years with good quality of life. The goal isn’t always cure-it’s slowing progression and keeping the heart working as long as possible.
Is pulmonary hypertension the same as regular high blood pressure?
No. Regular high blood pressure (hypertension) affects the arteries throughout the body and is measured in the arm. Pulmonary hypertension only affects the arteries between the heart and lungs. You can have normal blood pressure in your arm and still have dangerously high pressure in your lungs. They’re completely different conditions with different causes and treatments.
How do I know if my symptoms are PH and not asthma?
Asthma usually causes wheezing, chest tightness, and symptoms that improve with inhalers. PH causes progressive shortness of breath without wheezing, especially with activity, along with swelling in the legs, fatigue, and dizziness. If your breathing gets worse over months despite using asthma meds, or if you have signs like a bulging neck vein or right heart strain on echo, PH should be ruled out. A simple 6-minute walk test and echocardiogram can help differentiate.
What happens if PH is left untreated?
Without treatment, the right side of your heart keeps working harder until it fails. This leads to fluid buildup in the legs, belly, and lungs. You’ll feel constantly tired, dizzy, and short of breath-even at rest. Eventually, your heart can’t pump enough blood. Survival without treatment averages less than 3 years. Early diagnosis and therapy can extend life by decades.
Can I exercise with pulmonary hypertension?
Yes-but carefully. Regular, low-intensity exercise like walking or cycling helps maintain muscle strength and heart function. But intense activity or high-altitude environments can be dangerous. Always work with your PH care team. Many centers offer supervised pulmonary rehab programs. Avoid holding your breath, heavy lifting, or extreme heat. If you feel dizzy, chest pain, or extreme fatigue during exercise, stop immediately and contact your doctor.
about author

Anil bhardwaj
Been dealing with this for my mom-she’s 72, started getting winded just walking to the kitchen. Docs thought it was just aging. Took six months and a ER trip before someone even mentioned PH. Once they did, everything clicked. The swelling, the fatigue, the way she’d just sit there staring at the TV like she was too tired to think. This post nails it. No one talks about how sneaky this is.
Vanessa Drummond
Ugh. I hate how doctors just shrug and say 'get more sleep' or 'lose weight.' My sister had PH for 18 months before anyone checked her pulmonary pressure. She was 34. Active. No smoking. No obesity. Just… tired. And now she’s on IV meds. It’s not fair. Why do we wait until people are barely breathing before we take them seriously?
David McKie
Oh here we go again with the medical elitism. You act like PH is some mysterious conspiracy the system hides from us. Newsflash: most GPs aren’t cardiologists. They see 40 patients a day. If someone walks in saying 'I’m tired climbing stairs,' do you really think they’re going to order a right heart catheterization? That’s $10k+ and requires a specialist referral. You want to blame the system? Fine. But don’t act like every doctor is a villain who ignores symptoms on purpose. Some of us have been on the other side-waiting months for a slot at a PH center because the waitlist is 18 months long. It’s not malice. It’s broken infrastructure.
And don’t get me started on 'combination therapy.' You think it’s magic? Try getting insurance to cover three pulmonary drugs at once. I’ve seen patients skip doses because they can’t afford the copay. The real killer isn’t the disease-it’s the bureaucracy that turns treatment into a financial obstacle course.
And yes, I’ve sat in a PH clinic and watched a nurse cry because a patient’s BNP spiked and she couldn’t get the IV meds approved in time. That’s not negligence. That’s systemic failure. But don’t pretend your outrage changes anything. Only policy does.
lela izzani
As a nurse in a PH center, I see this every day. The 6-minute walk test isn’t just a number-it’s a mirror. One woman walked 310 meters last month. She cried because she used to walk her dog 2 miles. Now she can barely make it to the mailbox. We started her on triple therapy. Two months later? 470 meters. She smiled for the first time in a year. This isn’t hopeless. But it takes time, patience, and a team that doesn’t give up. If your doctor says 'it’s just asthma,' push back. Ask for echo. Ask for BNP. Ask for cath. You have a right to those tests.
Joanna Reyes
I’ve been researching PH for my husband since his diagnosis last year, and I can’t believe how little awareness there is-even among healthcare workers. We went to three different cardiologists before one even mentioned PH as a possibility. One said, 'You’re too young for this.' Another said, 'Try yoga.' The third, finally, ordered the echo and then the cath. We were lucky. Most aren’t. The fact that only 35 centers in the U.S. are certified is terrifying. And the cost? I spent 11 hours on the phone with insurance just to get sotatercept approved. We’re lucky we have good coverage. What about people without it? The system is failing them. And it’s not just about drugs-it’s about access to rehab, mental health support, home oxygen, transportation to appointments. No one talks about how exhausting this is for families. We’re not just caregivers-we’re case managers, financial advisors, and emotional anchors. And we’re doing it alone.
Stephen Archbold
Man, I read this and just… felt it. My cousin had PH. She was 28. Used to run marathons. Then she couldn’t walk to the bus stop. We thought she was depressed. Turns out her right ventricle was about to give out. She got on IV meds. Now she’s doing okay. But the system? Broke. Took 14 months to get her meds covered. She had to sell her car. I’m not mad. Just… heartbroken. We need better access. Not more science. More justice.
Southern Indiana Paleontology Institute
so like… ph is just high blood pressure in the lungs? duh. why is this even a thing? my grandpa had high bp and he lived to 89. maybe people just need to stop being lazy and start walking more. also, why are we spending 10k on cath tests? just give em a stethoscope and tell em to do squats. america is so soft.
Nerina Devi
I’m from rural India. We don’t have PH centers here. My aunt was diagnosed last year-she’s 54. She walks 5km to the nearest clinic every month for her meds. We don’t have echo machines in our town. She had to travel 300km to Hyderabad. No one told us about the 6-minute walk test. No one told us about BNP. We just knew she was tired. This post made me cry. We need education. Not just drugs. We need to teach nurses, village health workers, even schoolteachers-what to look for. Because in places like mine, the doctor is 100km away. The patient is the first line of defense.
Dinesh Dawn
My buddy had this. He’s 41. Thought he was just out of shape. Took him 18 months to get diagnosed. Now he’s on three meds. Still works. Still hikes. Still laughs. He says the biggest thing? Finding the right team. The nurse coordinator called him every week. Checked his labs. Adjusted his meds before he even felt bad. That’s the real hero. Not the drugs. The person who shows up.
Nick Hamby
There’s a philosophical layer here that often goes unspoken: the human body is not a machine to be fixed, but a system to be understood. Pulmonary hypertension reveals a profound truth-that our organs are not isolated, but deeply interdependent. The right ventricle doesn’t fail because of a single lesion; it fails because the entire circulatory narrative has been rewritten. We treat pressure as a number, but it’s a story of resistance, adaptation, and ultimately, collapse. The real breakthrough isn’t in the drugs, but in the shift from reactive care to anticipatory care. Can we detect right ventricular strain before symptoms arise? Can we measure microvascular remodeling before pressure climbs? The future lies not in louder alarms, but in quieter, earlier signals. And that requires humility-not just from clinicians, but from the entire medical paradigm.
kirti juneja
Just wanted to say-this is the kind of post that makes me believe in humanity again. I’m a community health worker in Kerala, and I’ve been handing out printed copies of this to local clinics. One old man came to me last week, said he’d been told his shortness of breath was 'just old age.' I showed him the part about TAPSE under 17mm. He cried. Said he’d been too ashamed to tell his kids he couldn’t carry his grandson anymore. We got him to the district hospital. Echo showed right heart strain. Cath confirmed PH. He’s on meds now. He’s walking again. This isn’t just medicine. It’s dignity. Thank you.